The described surgical techniques are recognized and approved by different scientifical societies; the general content of this website is approved and recommended by the BSCRS (Belgian Society of Cataract and Refractive Surgery) in its brochures concerning eye operations thanks to the work of several ophthalmologists The BSCRS counts 220 members, all ophthalmologists.
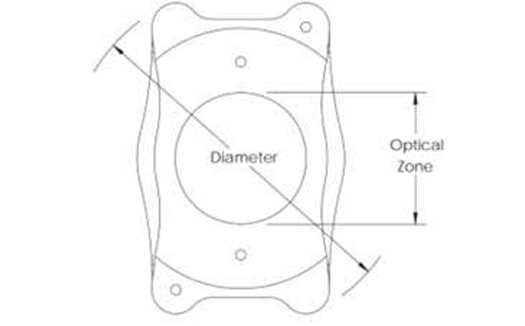
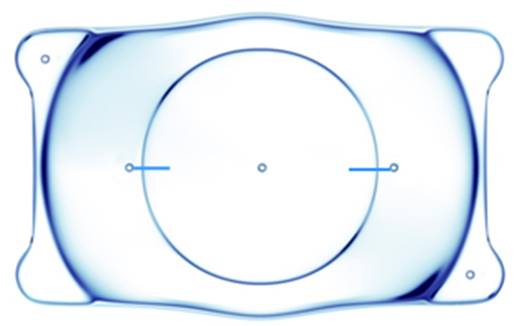
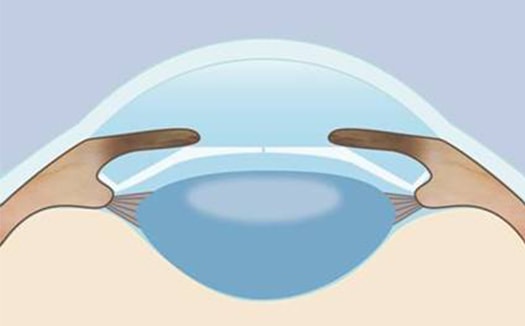
A special lens can be inserted in the eye to correct high refractive error, like high myopia, or more recently, high hyperopia. The concept of implanting another lens in the eye, without removing the crystalline lens, is not new and dates back from nearly 30 years. At that time, the materials used were not of the same quality as the ones we are using now, and despite this fact, the lens was well-tolerated. With the quality of the new optics, it is now possible to realize a very thin lens to be implanted in the posterior chamber of the eye (behind the iris: ICL) or in the anterior chamber (in front of the iris). Some lenses do really float behind the iris, or are fixated by small loops; other lenses will be attached to the iris by little claws.
The surgeon will advise his/her patient for the best lens in his/her case.
This surgery is performed in the operating room, under local of general anesthaesia, depending on the case. A careful eye examination will be conducted before the surgery, to check the depth of the anterior chamber of the eye, the corneal curvature, the retina, etc.
The major risks and complications of the surgery are: infection, glaucoma, retinal detachment, halos at night, over- and under correction. These complications are very rare. Moreover, with the new lenses, the risk of having a sight-threatening complication is very low, and the power of the lens can be calculated very accurately in most cases to avoid any refractive surprise.
This surgery is not reimbursed by the I.N.A.M.I. in Belgium, but some private insurances will consider it like any other surgeries.
A very effective and popular technique in the past, keratotomy is mainly used nowadays to correct small ametropia, or to improve the visual outcome after cataract surgery or another refractive surgery with low residual myopia or astigmatism.
Small incisions are performed under local anesthesia on the cornea, to obtain the desired effect of corneal flattening.
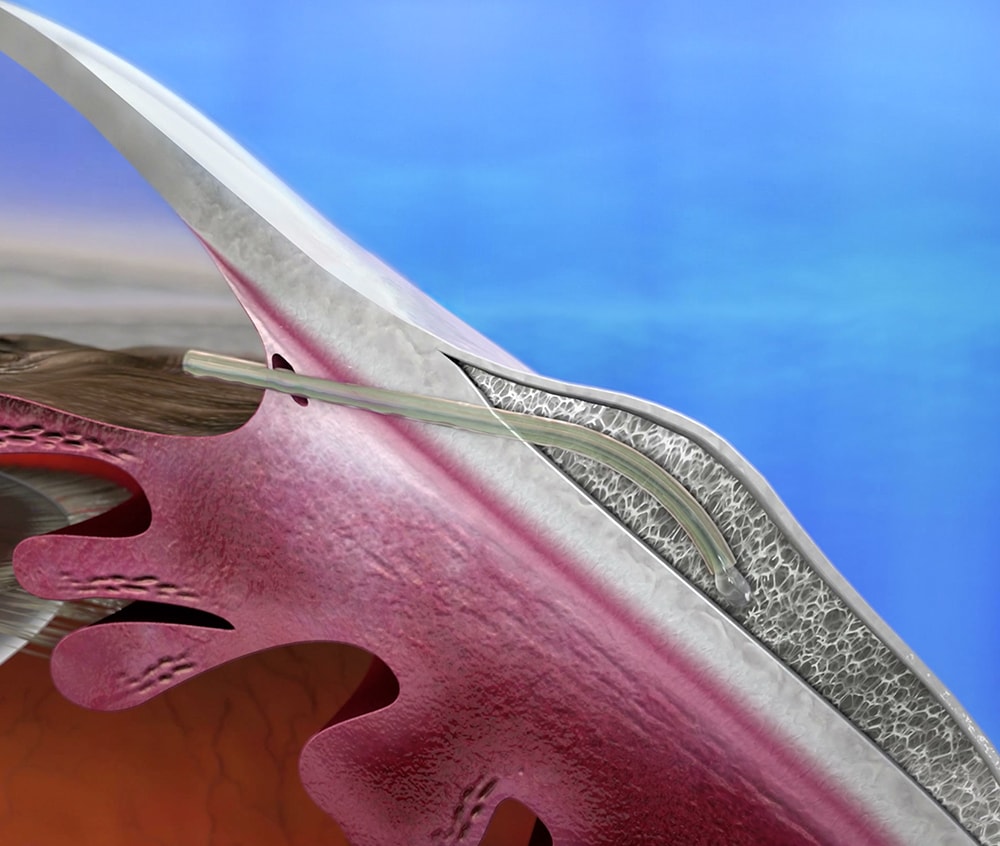
A new technique is the Stent. It is a small pipe (see diagram) implanted in the eye thanks to an injector. The intervention is performed under local anesthesia, ambulatory, and lasts a few minutes. It is a filtering intervention, allowing the flow of the aqueous humor, without having to resort to use the traditional intervention of trabeculectomy. The eye pressure is greatly improved and in most cases the antiglaucoma treatment may be interrupted because the intraocular pressure is normalized.
This procedure can be performed also in patients operated of cataract, or even be performed during the intervention of cataracts.
Once again, retinal holes, or tears in the peripheral retina will be treated by the laser; but in case of a retinal detachment, classical techniques must be used by a specialized surgeon, to restore the best possible visual acuity.
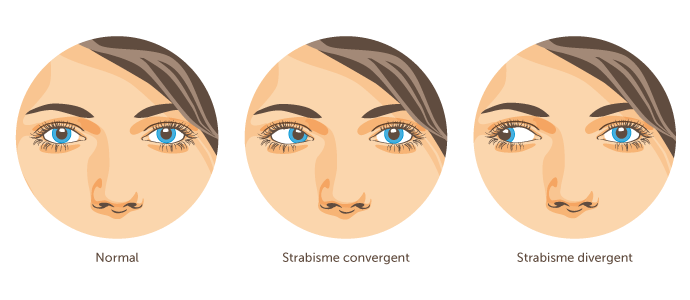
In order to correct the strabismus of a child, and sometimes the associated amblyopia, one can operate on the muscles of the eye and move them slightly. Some adults are operated only for cosmetic reasons.
To be performed when the free edge of the eyelid bends inwards (entropion) or outwards (ectropion). The eyes are then irritated by the rubbing of the eyelashes, or by the gaping palpebral opening. Blepharochalasis (excess skin in the upper eyelid) can also be treated.